COVID-19 백신 접종 후 발생한 백혈구파쇄혈관염 1례
A Case of Leukocytoclastic Vasculitis Following COVID-19 Vaccination
Article information
Trans Abstract
As the coronavirus disease 2019 (COVID-19) vaccination rate has recently risen, various cutaneous adverse events have been reported. We report on a 75-year-old woman who developed leukocytoclastic vasculitis after the first dose of BNT162b2 (Pfizer, United States of America) vaccine. The cause of leukocytoclastic vasculitis can be idiopathic or secondary to medications, infections, connective tissue disorders, and malignancy. Developing and exacerbation of leukocytoclastic vasculitis has been reported following vaccinations such as influenza, hepatitis B virus, and bacillus Calmette-Guerin vaccine. The pathogenesis might involve hyperactivation of the immune system secondary to cross-reactivity and molecular mimicry between the virus and self-antigens. As it is important to consider COVID-19 vaccine as a cause of leukocytoclastic vasculitis, we report a case of leukocytoclastic vasculitis following COVID-19 vaccination.
Introduction
최근 coronavirus disease 2019(COVID-19) 백신 접종률이 증가함에 따라 다양한 피부 부작용(Cutaneous adverse events)이 보고되고 있으며, 지연형 국소반응(delayed large local reaction), 국소주사부위반응(local injection site reaction), 두드러기, 수포성 유천포창양(Bullous pemphigoid-like), 홍역모양 반응(morbilliform reactions), 홍색사지통증(erythromelalgia), 대상포진 (herpes zoster lesion), 혈관염(vasculitis), 동창(chilblains) 등의 피부 반응이 흔히 보고되었다[1,2]. 저자는 COVID-19 백신 접종 후 피부 반응이 동반되어 발생한 백혈구파쇄혈관염(Leukocytoclastic vasculitis) 1례를 경험하여 문헌고찰과 함께 보고하는 바이다.
Case
75세 여성이 양측 하지 및 체간에서 통증과 소양감을 동반한 적자색의 자반성 반점 및 반을 주소로 내원하였다(Fig.1). 내원 7일전 BNT162b2 COVID-19 백신(Pfizer, United States of America) 접종하였고, 하루 뒤인 내원 6일전 양측 하지에 자반이 발생하였으며 설사와 복통이 2일간 지속된 뒤 내원 4일전 자반이 체간으로 넓어지며 악화되어 내원하였다. 내원 당시 설사와 복통은 없었으며 우측 고관절통을 호소하였다.

Multiple reddish to violaceous confluent patches and macules on both lower legs. (A) Anterior view. (B) Posterior view. (C) Closed-up view.
과거력상 고혈압으로 약물 복용 중이었으며 기존 고혈압 약제 외 약물 복용력은 없었다. 신체검사에서 피부소견 외 특이소견은 없었다. 일반혈액검사에서 적혈구침강속도 42 mm/hr, C-반응성단백 0.6 mg/dL로 증가되어있었고 혈액응고검사에서 섬유소원분해산물 14.5 μg/mL, D-이합체 3.77 μg/mL로 증가되어있었다. 자가면역 관련 항체검사에서 항핵항체 1:160으로 양성 외 특이소견은 없었고 면역글로불린 및 보체검사에서도 특이소견은 없었다. 그 외 신장, 간 기능검사 및 소변검사에서도 특이소견은 없었다. D-이합체 상승에 대한 검사를 시행하려 하였으나 환자가 동의하지 않아 시행하지 못하였다. 우측 하지에서 시행한 병리조직검사상 저배율에서 진피의 혈관 주위로 염증세포의 침윤이 관찰되었으며, 고배율에서 주로 호중구와 때때로 림프구 및 호산구로 구성된 염증세포의 침윤, 혈관벽의 괴사와 섬유소 침착, 적혈구혈관외유출과 핵먼지가 관찰되었다(Fig.2). 면역형광염색에서 IgG, IgA, IgM, C3, 섬유소원 침착은 관찰되지 않았다. 이상의 임상 및 병리조직학적 소견을 바탕으로 COVID-19 백신에 의한 백혈구파쇄혈관염으로 진단 후 전신스테로이드, 항히스타민제 및 국소스테로이드제재를 사용하였고 입원 6일째 병변부가 어두워지며 호전을 보여 퇴원하였다. 이후 외래에서 치료를 지속하여 3주에 걸쳐 대부분 피부병변이 호전되었고, 2차 백신접종 후 증상 재발 없이 현재까지 경과 관찰 중이다.
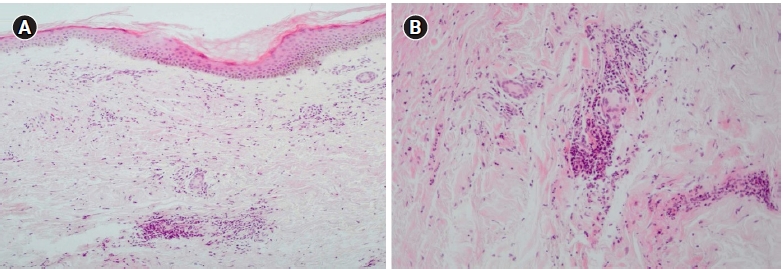
(A) Histopathologic finding perivascular inflammatory infiltration (H&E, ×100). (B) Perivascular mixed inflammatory infiltrate with numerous neutrophils, lymphocytes and occasional eosinophils, vascular necrosis and fibrin, erythrocyte extravasation and nuclear dust in the dermis (H&E, ×200).
Discussion
백혈구파쇄혈관염의 원인은 대부분 미상이며 50%정도는 약물과 감염에 의한 것이나 결체조직질환이나 악성종양과 관련하여 발생하기도 한다[3]. 인플루엔자바이러스, B형간염바이러스, bacillus Calmette-Guerin 등의 백신 접종 후 혈관염이 발생한 사례들이 보고된 바 있으며 백신항원과 자가항원의 교차반응에 의한 면역활성이 그 기전으로 추정된다[4]. COVID-19 백신 접종에 의한 백혈구파쇄혈관염의 원인은 아직까지 명확히 밝혀진 바 없다. 그러나 COVID-19의 원인 바이러스인 severe acute respiratory syndrome coronavirus 2(SARS-CoV-2)가 교차반응과 분자모방를 통해 과도한 면역반응을 일으킬 수 있다고 알려져 있으며, SARS-CoV-2 spike 당단백질을 암호화하는 백신의 성분이 이와 유사한 면역반응을 통해 면역복합체를 형성해 혈관염을 일으키는 것으로 추정된다[5].
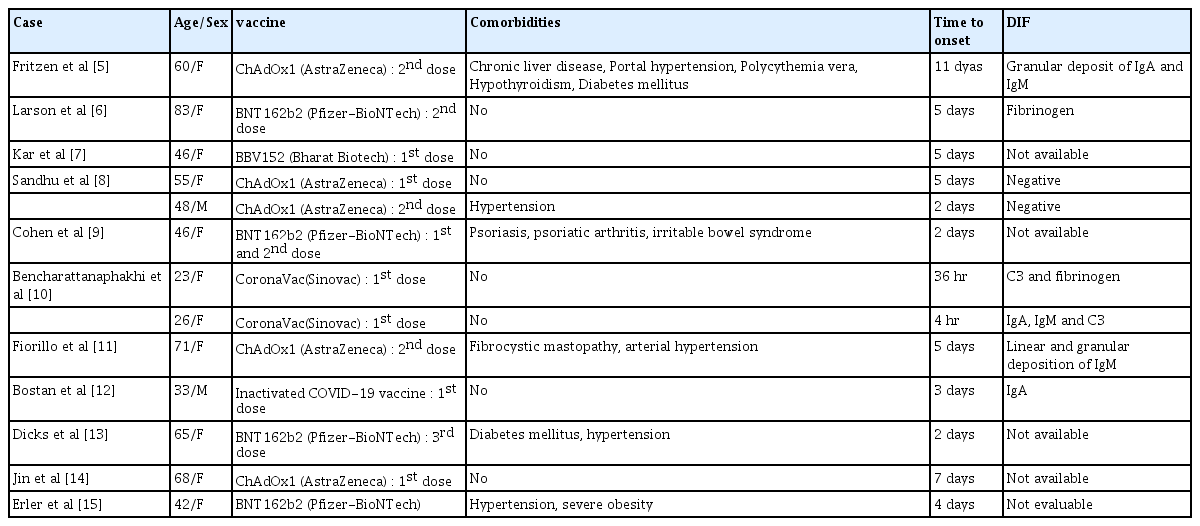
COVID-19 백신 접종 후 발생한 백혈구파쇄혈관염의 경우 국외에서 12례, 국내에서는 1례만 보고되었다(Table 1). 미국피부과학회(American Academy of Dermatology)의 registry를 기반으로 한 임상양상만으로 COVID-19 백신 접종 후 피부 부작용을 분류한 연구에서는 총 3례의 혈관염이 보고되었다 [1]. 2례는 mRNA-1273 COVID-19 백신(Moderna, United States of America) 접종 후 발생하였고 이는 첫번째 mRNA-1273 백신 접종 후 보고된 피부반응의 0.7%에 해당하였다[1]. 나머지 1예는 BNT162b2 백신 접종 후 발생하였고, 첫번째 BNT162b2 백신 접종 후 보고된 피부반응의 2.9%에 해당하였다[1]. 이후 registry에 등록된 사례 중 조직 생검을 시행한 경우만 모아서 연구해 보았더니 총 58건 중 2건에서 백혈구파쇄혈관염의 소견이 관찰되었다[2].
Summary of published cases of leukocytoclastic vasculitis following COVID-19 vaccination
본 증례는 피부병변 외 설사를 동반한 복통과 우측 고관절통을 호소하여 IgA혈관염과의 감별이 필요하였으나 면역형광염색검사에서 IgA 침착이 관찰되지 않아 배제할 수 있었다. 현재까지 보고된 COVID-19 백신 접종 후 발생한 백혈구파쇄혈관염 증례들의 경우 백신 접종 후 4시간에서 11일 사이에 발생하였는데(Table 1), 본 증례에서도 COVID-19 백신 접종 하루 뒤 피부 병변 발생하였으며 최근 변경된 약제 및 감염의 증거가 없고 고혈압 외 기저질환이 없으므로 COVID-19 백신 접종에 의한 백혈구파쇄혈관염으로 진단을 내렸다.
이에 저자들은 COVID-19 백신 접종 후 발생한 백혈구파쇄혈관염 1례를 경험하고 COVID-19 백신 접종 후 유사한 임상양상을 보이는 경우 고려해보아야 할 원인이라 생각되어 보고하는 바이다.
Notes
Conflict of interest
The authors declare no conflicts-of-interest related to this article.