


Introduction
Subcutaneous panniculitis-like T-cell lymphoma (SPLTCL) which is similar to lobular panniculitis is a subtype of skin lymphoma that is characterized by pleomorphic T cells and benign macrophages which infiltrates to subcutaneous tissue. The simultaneous presence of hemophagocytic lymphohistiocytosis is the most important and adverse prognostic factor in SPLTCL [1]. SPLTCL is a rare disease with no well-established standard treatment. Various protocols have therefore been used. Successful treatment of SPLTCL with hemophagocytic lymphohistiocytosis (HLH) in children has rarely been reported [2ŌĆō4].
We present a case of SPLTCL with HLH successfully treated initialy with dexamethasone and etoposide followed by modified NHL (non-Hodgkin lymphoma)-BFM(BerlinŌĆÉFrankfurtŌĆÉM├╝nster)-90 and HLH-2004.
Case report
An eight-year-old boy was admitted to the department of pediatric surgery with a two-week history of fever and an abdominal mass. He continued to be febrile with intravenous antibiotics, and because of bicytopenia, he was transferred to the department of pediatrics.
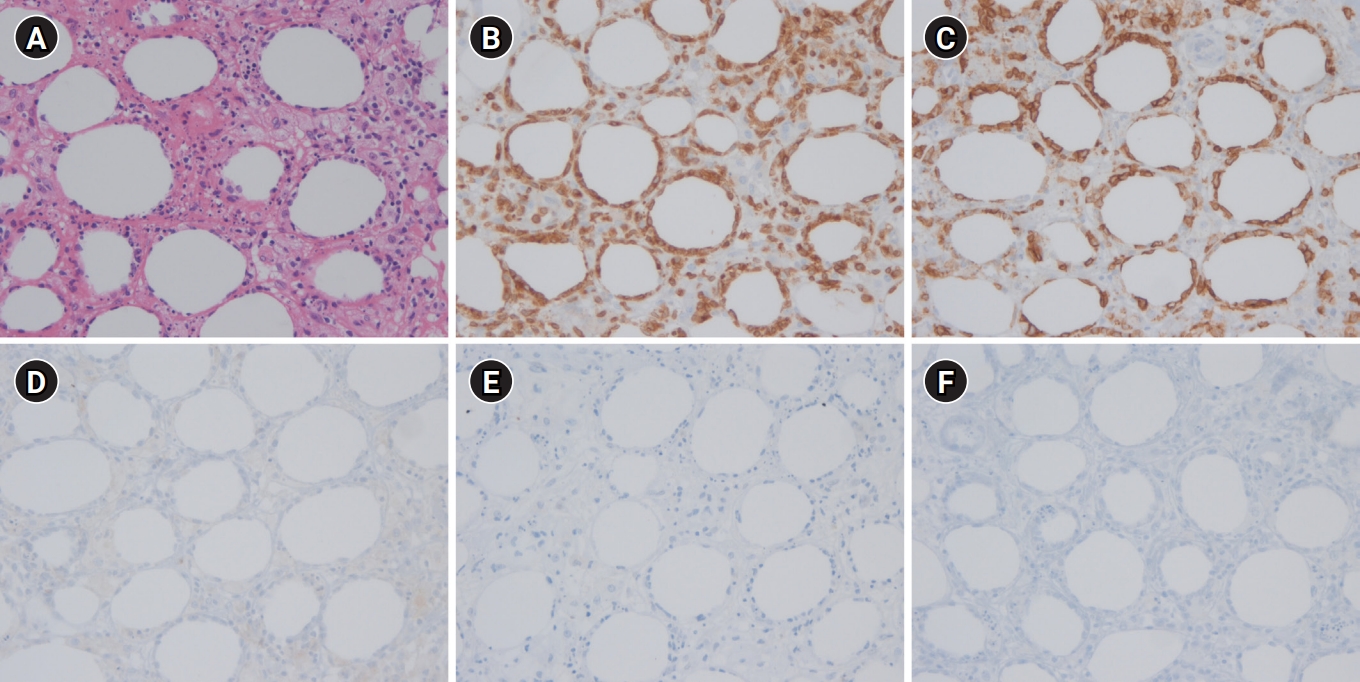
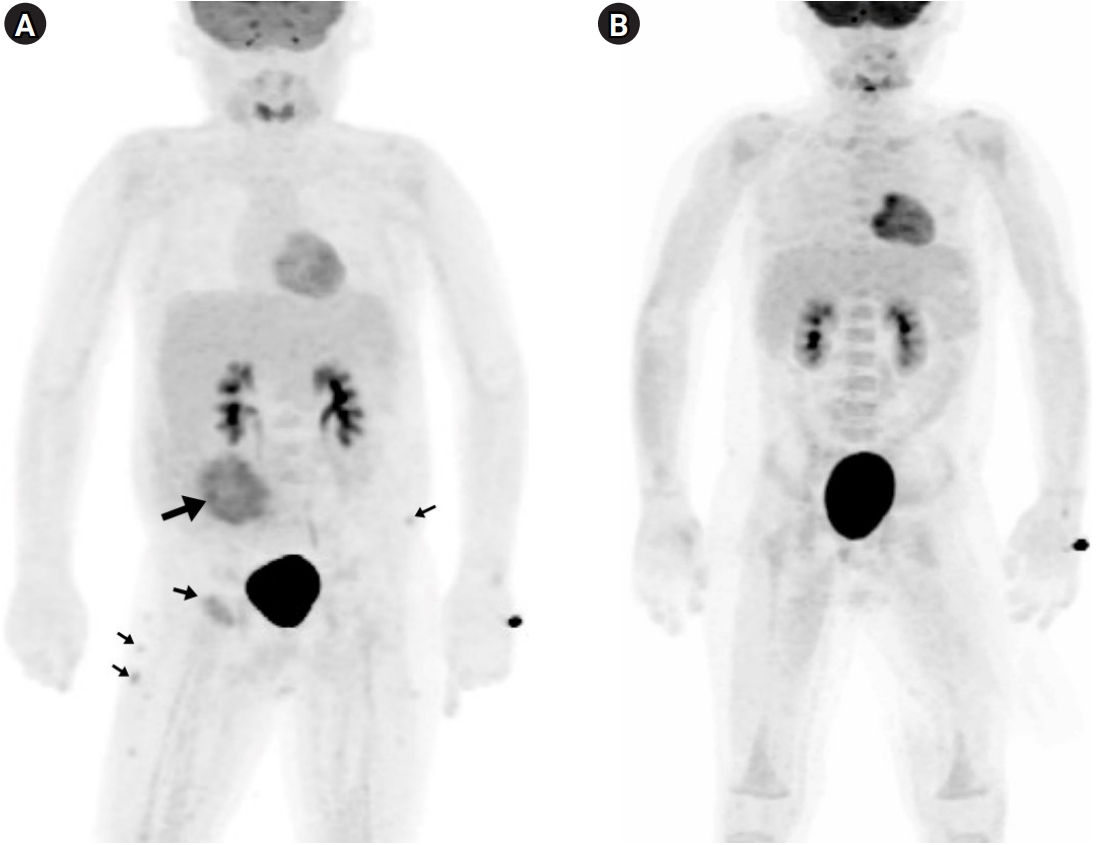
On physical examination, a tender, 15 cm round erythematous swelling on right mid-abdominal wall (Fig. 1) and hepatosplenomegaly (subsequently confirmed by computed tomography) were observed. Initial laboratory findings were: white blood cell count, 2.4├Ś109/dm3; hemoglobin, 99 g/dm3; platelet count, 147├Ś109/dm3; C-reactive protein, 275.24 nmol/dm3 (normal: 0.0ŌĆō47.62 nmol/dm3); triglycerides, 4.16 mmol/dm3 (normal: 0.56ŌĆō1.47 mmol/dm3); fibrinogen, 1.7 g/dm3 (normal: 2.0ŌĆō4.0 g/dm3); soluble interleukin 2 receptor, 14,991 pg/cm3 (normal: 1,398ŌĆō5,513 pg/cm3); ferritin, 1,126.52 pmol/dm3 (normal: 33.71ŌĆō449.44 pmol/dm3) and EpsteinŌĆōBarr virus and cytomegalovirus immunoglobulin titers, negative. Biopsy of the abdominal mass showed subcutaneous infiltration by atypical lymphocytes rimming adipocytes. Immunohistochemistry of the specimen was positive for CD3 and CD8, and negative for CD4, CD20, and CD56 (Fig. 2). T Cell receptor (TCR) gene rearrangement analysis revealed ╔Ż oligoclonality. Whole-body 18F-fluorodeoxyglucose positron emission tomography (PET) revealed increased contrast uptake in subcutaneous tissues of the right abdominal wall, left anterior chest wall, right upper quadrant abdominal wall, left pelvis, bilateral buttocks, and upper legs (Fig. 3). Taken together, these results led to a diagnosis of SPLTCL with HLH.
Treatment with dexamethasone and etoposide was started immediately, and the patient defervesced the next day. After four weeks of HLH induction therapy with dexamethasone and etoposide, NHL-BFM-90 course A was started. When serum ferritin subsequently became elevated above 4,494.38 pmol/dm3, we considered the possibility of HLH aggravation. Thus, four weeks of HLH-2004 induction treatment was repeated with dexamethasone, etoposide, and added cyclosporine A. Thereafter, per protocol, NHL-BFM-90 courses B-A-B-A-B were administered, leading to complete remission with normalized PET results. High ferritin persisted (up to 3,315 pmol/dm3), however. The sustained ferritin elevation was worrisome and suspicious for incomplete control of HLH. A maintenance course of HLH-2004 was therefore continued for a total of 40 weeks. The tumor necrosis factor ╬▒ (TNF- ╬▒) inhibitor etanercept was then administered for a further year. On regular follow-up, the patient has been doing well, except for a ferritin level of approximately 2,247 pmol/dm3.
Discussion
SPLTCL is a type of skin lymphoma characterized by pleomorphic T cells and benign macrophages that infiltrate to subcutaneous tissue, mimicking lobular panniculitis [3]. It is characterized by cutaneous plaques and nodules which are slowly progressive and have a tendency to ulcerate.
SPLTCL is divided into two subtypes: ╬▒/╬▓ and ╬│/╬┤. In 2005, the World Health Organization (WHO) and European Organization for Research and Treatment of Cancer (EORTC) classification of primary cutaneous lymphomas has restricted the category of SPLTCL to tumors expressing the TCR ╬▒/╬▓, CD4-, CD8+, CD56-. Cutaneous ╬│╬┤ T-cell lymphoma was restricted that expressing the TCR ╬│/╬┤, CD4-, CD8- [1]. This categorization was based on the differences in prognoses between these two, with SPLTCL showing much favorable clinical outcomes [5].
Gayden et al [6] reported in their, recent studies on the cases showing familial predisposition by gene mutation as one of the causes of SPLTCL and HLH. TIM-3, a gene likely related to SPLTCL, is a transmembrane protein expressed by CD8+ T cells and natural killer cells, and a negative immune checkpoint through interactions with cognate ligands included galectin-9 [6,7]. Tyr82Cys and Ile97Met at TIM-3 are the most commonly found mutations in SPLTCL. These two variants induce protein misfolding and membrane expression failure in T cells and monocytes, leading to persistent immune activation and increased production of inflammatory cytokines, promoting SPTCL and HLH [6]. Thus, these authors insisted to consider that immunosuppression and more novel agents targeting IL-1 and IFN-╬│ when the TIM-3 mutation is identified in children with SPLTCL and HLH [6].
The prognosis is poor in malignany-related HLH [8]. Probably the treatment intensity could have been too intensive for induction period. When HLH and malignancy are accompanied, the delay in the diagnosis of HLH due to clinical similarity may also be a contributing factor [9].
Standard therapeutic options for SPLTCL have not been established, and protocols as various as CHOP (cyclophosphamide-vincristine-doxorubicin-prednisolone), SMILE (steroid, methotrexate, ifosfamide, L-asparaginase, and etoposide), NHL-BFM-90, and stem-cell transplantation have been tried [2,4]. CHOP has recently been reported to have little effect. SPLTCL with HLH is a rare disease in children. NHL-BFM-90 was demonstrated to result in relatively good long-term responses with acceptable toxicity in combined SPLTCL and HLH [3,4].
We suspected the present case of SPTCL accompanying HLH. We reviewed the literature of SPLTCL with HLH in children to determine the treatment options for the patient (Table. 1).
Among 11 reported cases, 5 cases were treated with NHL-BFM-90 protocol, 2 cases with CsA and steroid, 2 cases with CHOP and 1 case each with SMILE or CEOP (cyclophosphamide, epirubicin, vincristine, and prednisone). All of NHL-BFM-90 based protocol induced remission. Among 2 cases of patients treated with CHOP, 1 case was induced in remission and another case was expired.
We selected the combination of the NHL-BFM-90 and HLH-2004 protocols. However, when we analyzed the causes of failed cases, most of them expired during initial induction period, indicating that the intensity of the initial treatment might have been too intensive [8].
In addition, treatment of malignant diseases with HLH are known to show no universal conclusions due to lack of large samples or prospective clinical trials [9]. We started dexamethasone and etoposide as these two drugs are included in NHL-BFM-90 and HLH-2004 protocols. We expected these two drugs would work for HLH as well as SPLTCL and not aggravate stormy cytokine reaction. After induction period, when HLH features were improving and subcutaneous masses were decreasing in size, we used anticancer drugs in the NHL-BFM-90 protocol fully.
After complete resolution of the subcutaneous lesions as well as the most features of the HLH were resolved, hyperferritinemia persisted. We had suspicion of incompleted control of HLH related hyperferritinemia [10]. Thus, we tried etanercept which is known to inhibit the activity of TNF- ╬▒ by competitively binding with its cell-surface receptors for further control of HLH [11]. Etanercept has been reported to be useful for controlling inflammatory cytokines in therapy-resistant macrophage activation syndrome [11]. The pathophysiology in secondary HLH and macrophage activation syndrome seems to be similar, with excessive immune activation and hemophagocytosis [11]. Takahashi et al [12] successfully treated lupus-associated HLH with etanercept. Thus, we administered etanercept as an immune system mediator to regulate TNF- ╬▒. Administration of etanercept led to moderately decreased serum ferritin, but it did not produce a response as dramatic as we had expected.
In summary, we report a case in which the modified NHL-BFM-90 and HLH-2004 protocols were applied in a child of SPLTCL with HLH, and successfully treated. We tried etanercept to reduce high serum ferritin, with some effect. Thus, further studies are needed for unresolved hyperferritinemia. In children with diagnosis of SPLTCL with HLH, initiation of immediate treatment affects prognosis. Prompt initiation of agents such as dexamethasone and etoposide that can simultaneously control underlying disease as well as secondary HLH could lead to successful results.