

Introduction
In China since the outbreak of COVID-19 in December 2019, the resulting pandemic has inflicted 6,251,567 deaths worldwide as of 10 May 2022.
In Northeast Asian areas including Korea and Japan, the situation of COVID-19 differs based on the governmentsŌĆÖ policies, people's attitudes, and the rate of vaccination implementation [1, 2].
In this overview, the incidence of COVID-19 infection between Korea and Japan is compared, focusing on three periods: 2020.1~2021.10, 2021.11~2021.12, and 2022.1~2022.4.
COVID-19 infection in Korea and Japan between 2020.1~2021.10.
The first cluster in Korea occurred in Daegu City in February 2020.
The excellent and sophisticated and collaborative efforts by medical staff, civil servants, and the heroic stance of the citizens in Daegu City brought about the least number of victims. Vivid and impressive reports [3-7] were published which helped other Korean areas to prevent as much as possible the damage by COVID-19.
Thus, the Daegu protective measures became the prototype of Korean (K) protection.
Irrespective of the COVID-19 cluster (more than seven hundred infected persons) at a church in Daegu City in February 2020, the containment of COVID-19 in Korea has been relatively well implemented between March 2020 and October 2021.
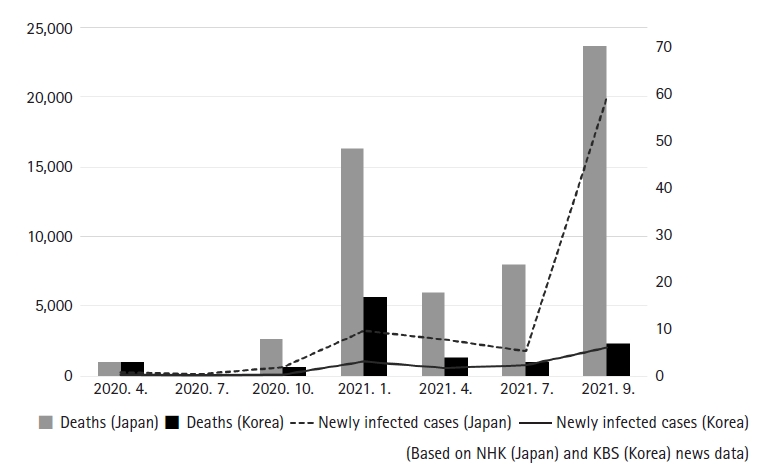
The number of newly infected cases and deaths in Korea and Japan is shown in Fig. 1.
The number of newly infected cases was as follows.
As of April 2020, 101 in Korea, 268 in Japan.
As of October 2020, 77 in Korea, 633 in Japan.
As of April 2021, 551 in Korea, 2,605 in Japan.
The number of deaths in Korea and Japan, respectively, was as follows (Fig. 1).
As of April 2020, 3 and 3.
As of October 2020, 2 and 8.
As of April 2021, 4 and 18.
By population, the incidence of COVID-19 infection in Korea had always been lower than in Japan, and is attributed to the so-called K protection.
K protection was between March 2020 and October 2021 considered an excellent model against COVID-19 in the world. Its contributing factors being as follows:
First, learning from the experience with Middle East Respiratory Syndrome (MERS) contracted by 40 persons in 2015 [8].
Second, the precise assessment of infected persons by thorough PCR examination.
Third, the comprehensive triage policy, including intensive care, for severely affected persons and health-maintaining care for mildly affected persons.
Fourth, the dedicated efforts of medical staff.
Fifth, cooperation of the citizens in the mandated practices set by the government.
COVID-19 infection in Korea and Japan between 2021.11~2021.12
The situation had changed, however, since November 2021.
The weekly increase in the number of newly infected cases rose from 1,735 in October to 6,097 (3.5-fold) in December.
Hospitalized cases increased from 332 on 31 October to 875 (2.6-fold) on 13 December.
Deaths per week increased from 12 in October to 57 (4.8-fold) in December.
The main reason for this increase was attributed to the so-called "with corona" policy adopted by the government [9].
The government relaxed the restriction on gatherings, irrespective of opposition by medical experts. Another reason for the increase in the number of COVID-19 was attributed to overevaluation of the protection of vaccinations against COVID-19 [9]. According to the government report, the decrease in the titer of neutralizing antibodies, especially for elderly people, was very clear.
For example, the titer of neutralizing antibodies two weeks and three weeks after AstraZenecaŌĆÖs vaccine dropped to 392-fold and 146-fold, respectively, compared with 2,852-fold after ModernaŌĆÖs vaccine, and 2,119-fold after PfizerŌĆÖs vaccine.
In cross-vaccination, AstraZenecaŌĆÖs vaccine (first shot) and PfizerŌĆÖs vaccine (second shot), the titer of neutralizing antibodies dropped to 326-fold, whereas after Pfizer's vaccine (first shot) and AstraZenecaŌĆÖs vaccine (second shot) the titer dropped to 865-fold.
The data in terms of Moderna's vaccine were not reported [9].
That resulted in the remarkable increase in newly infected cases and deaths.
During the same period (2021.10~2021.12), the number of newly infected cases per day dropped dramatically to less than 1,000 in Japan, the so-called "golden period", explained by the high rate of the implementation of two-time vaccination and adherence to the restrictions set in Japanese society.
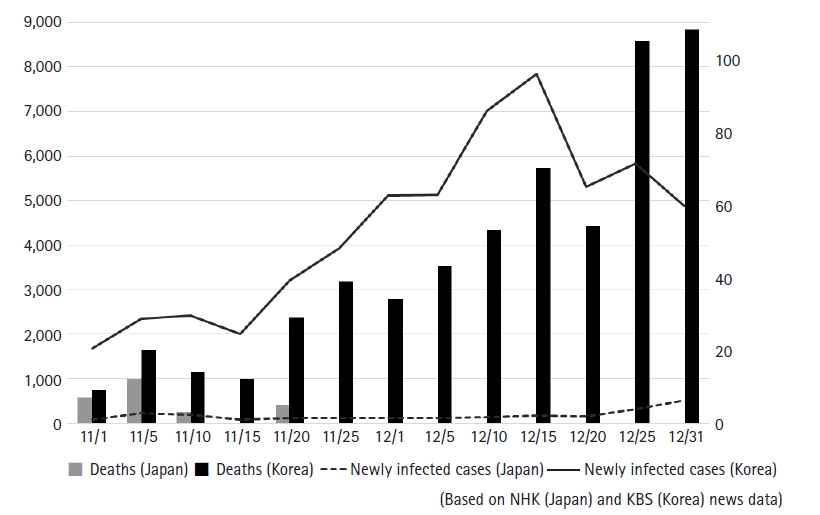
The number of newly confirmed infections and deaths in the two countries is shown in Fig. 2.
As of November 1 2021, newly confirmed infections stood at 1,684 in Korea and 84 in Japan, 9 deaths in Korea and 7 in Japan.
As of December 1 2021, newly confirmed infections stood at 5,122 in Korea and 119 in Japan, with 34 deaths in Korea, and none in Japan.
COVID-19 infection in Korea and Japan between 2022.1’Į×2022.4
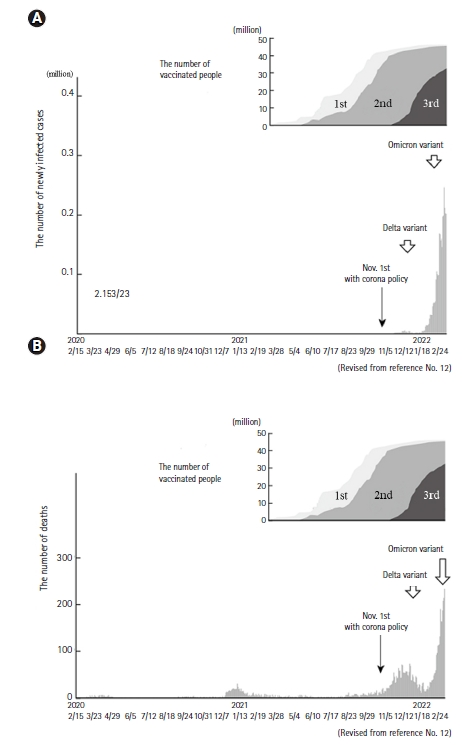
From January 2022, the Omicron variant (BA1 and BA2) of COVID-19 became prevalent in both countries (Fig. 3) [10,11].
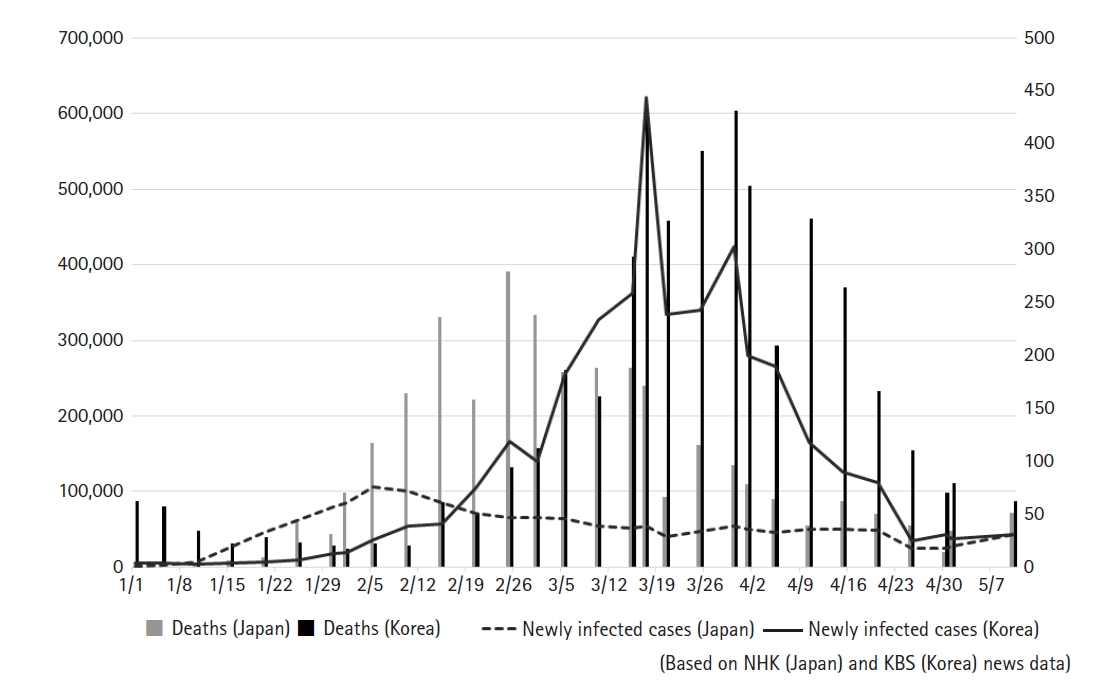
The number of newly confirmed infections and deaths in the two countries is shown in Fig. 4.
Under the ŌĆ£with corona policyŌĆØ, an infection explosion occurred in Korea, irrespective of the implementation of a high rate of vaccination, which accounted for 80% of two-time vaccination in the general population and 80% of three-time vaccination in the elderly population. Especially, since 12 March, over 300,000 people were infected consecutively every day (Fig. 3A) [12].
Almost 620,000 people were infected on 17 March.
However, Korean people including medical professionals and the general population did not consider that the ŌĆ£with coronaŌĆØ was necessarily a failure, because the number of deaths was relatively low compared with the number of newly infected cases (Fig. 3B).
The paradoxical fact such as high infection rate and relatively low death rate was explained by the high rate of vaccinations in the general population, especially in the elderly population.
In contrast, about less than 100,000 infected people per day continued between 2022.1 and 2022.4 in Japan, a relatively low level compared with the infected people in Korea. (Fig. 4)
That was explained by the high rate of vaccinations and adherence to restrictions such as prohibition of three Cs (closed spaces, crowded places, close-contact settings) in Japanese society. [12]
The number of newly infected cases was as follows: (Fig. 4)
As of 15 January 2022, 4,420 in Korea, 25,730 in Japan.
As of 15 February 2022, 57,147 in Korea, 84,195 in Japan.
As of 17 March 2022, 621,178 in Korea, 53,557 in Japan.
As of 15 April 2022, 125,800 in Korea, 49,738 in Japan
The number of deaths was as follows: (Fig. 4)
As of 15 January 2022, 22 in Korea, 6 in Japan.
As of 15 February 2022, 61 in Korea, 236 in Japan.
As of 17 March 2022, 429 in Korea, 171 in Japan.
As of 15 April 2022, 264 in Korea, 62 in Japan.
Regarding North Asian areas such as Korea and Japan, the incidence of COVID-19 and the rate of two-time vaccination implementation in England and Israel were also compared, where the Omicron variant became prevalent since November 2021.
The number of newly infected cases was as follows. (Cited from Johns Hopkins University's data)
As of 17 March 2022, 90,974 in England, 4,766 in Israel.
The number of deaths was as follows.
As of 17 March 2022, 153 in England, 6 in Israel.
The rate of two-time vaccination implementation in England and Israel were as follows.
As of 13 January 2022, 65% each of the general population in England and Israel [12].
Conclusion
Since the outbreak of COVID-19, the number of infections has been different between Korea and Japan in terms of the number of newly infected cases and the number of deaths. The situation seems to be associated with governmentsŌĆÖ policies, peopleŌĆÖs attitudes, and the rate of vaccination implementation.
The Japanese situation of COVID-19 is characterized as relatively stable over two years, explained especially by the adherence to the social restrictions set by the citizens, irrespective of inconsistent government policy.
The Korean situation of COVID-19 is, however, characterized by the remarkable contrast between 2020.2~2021.10 and 2021.11~2022.4, as explained especially by the change in government's ŌĆ£with corona policyŌĆØ.
Currently, it is difficult to conceive of absolute containment of COVID-19 in the near future. Nonetheless, a breakthrough including development of all-round vaccination and effective drugs against COVID-19 could be foreseen in the long run.
Probably, the process of containment of COVID-19, would differ between the two countries. Mutual communication of containment processes, however, would be needed between the two countries to attain COVID-19 containment, which may lead to achieving COVID-19 containment not only in North Asian areas but also all over the world.